
Integrating Physical and Mental Health in Tanzania Village Wellness Programs

On the first service program back to Tanzania following the pandemic lockdown, the Reaching Children’s Potential Program (RCP) launched a mental wellness initiative aiming to extend care, education and support through workshops, home visits, group meetings and clinical examinations and assessments. With broad acceptance and endorsement by community and church leaders throughout the Ukwega Ward, RCP parents are encouraged to share their questions, needs and concerns with volunteer professionals, RCP caregivers and clinic staff so treatment options for behavioral health may be developed and improved. Read on to learn about the state of mental health in Tanzania and needs in Global Volunteers’ partner communities.
By Global Volunteers Co-Founder Michele Gran
Not much is published on the current state of behavioral health services in Tanzania. Historically, improvements to the nation’s mental health services have been hindered by various factors at several levels, including limited healthcare facilities with mental health capacity, lack of funding and information technology, and poor educational and informational outreach, most especially in rural areas. In general, services for mental health in Tanzania still face many complex challenges.
More than 70% of Tanzania’s 62 million residents live in the rural areas, with about 36% surviving below the national poverty level. Data for the population living with mental health-related needs is limited in 2021. According to the World Health Organization (WHO), only 0.04 psychiatrists and 0.005 psychologists per 100,000 population are available to the country’s people, with the fewest accessible in rural areas. Overall, only 0.3 mental health workers (including psychologists, psychiatrists, nurses, and other mental health providers) are available per 100,000 population. This leaves those with needs for better mental health in Tanzania vulnerable.

The U.N. Sustainable Development Goal (SDG) #3, “Ensure Healthy Lives and Promote Wellbeing”, reinforces WHO’s definition of health, specifically that as a holistic concept, mental health must be integrated into primary health care. In September 2015, the United Nations General Assembly included mental health and substance abuse in SDG #3, marking the first time world leaders recognized mental health as a global priority. However, African countries currently dedicate on average less than 1% of their health budgets (themselves minuscule) to mental health, compared with 6–12% in Europe and North America, according to WHO. The Mental Health Innovation Network (MHIN) states: “The challenge is compounded by the fact that in most societies, mental illness is still widely stigmatised, inhibiting both sufferers and their families from admitting the condition and seeking help.”
“A bigger effort is needed to train health workers to recognise the symptoms of mental health problems and recommend appropriate treatment. The enormous range of mental health problems needs to be recognised, from relatively common conditions such as stress, anxiety and depression, to more serious conditions that can cause severe disability, such as schizophrenia.”
Mental Health Innovation Network
The widely held view in Africa that mentally ill patients caused their condition by using illicit drugs may be one reason state governments do not prioritize mental health. Experts have also cited African beliefs of acute mental health diseases as supernatural afflictions that can be cured only through spiritual or traditional interventions, such as “prayer camps” where individuals are subjected to violent rituals.
Mental Health in Tanzania: Diagnosis and Treatment
Mental health services in Tanzania are provided under the Ministry of Health, Community Development, Gender, Elderly and Children. The Tanzania health sector is centrally organized, with the parent ministry monitoring and coordinating national health priorities and plans, and the regional and district hospitals implementing those priorities. Organizationally, the health sector is hierarchically organized into national, regional, district and health centers and dispensaries at the village level. In most regions, there are only 20 beds for a population of 1.5 million people, making mental health treatment in Tanzania largely inaccessible.

Particularly in rural areas, local people lack awareness of mental illness as a medical condition which can be treated. The human rights of those with such diagnoses are subjected to outdated laws, resulting in violations in all all areas of life, including access to care, employment, security, and protection from harm. As throughout the rest of Africa and the world, mental illnesses are deeply stigmatized, resulting in only a small percentage of individuals seeking needed care. WHO estimates Tanzania spends only about 0.05% of its health budget on mental health, and most of this – about 70% – is spent in the largest urban areas.
Although 1 out of every 4 people in the world will be affected by mental or neurological disorders, in developing countries, up to 85% of people receive no treatment for their conditions. Barriers to care include fear, ignorance, stigma, inaccurate diagnosis, and lack of access to medical resources and trained healthcare providers. Those who live in poverty, amidst conflict and political oppression, or within areas of natural/environmental destruction are particularly prone to an array of mental and behavioral stresses and illness. Physical illness can compound mental illness and vice versa. Mental illness is one of the top causes of disability in all cultures.
Furthermore, such conditions can lead to poor nutrition and hygiene, and prenatal damage during early fetal brain development or trauma that occurs at the time of birth – extending mental illnesses to the next generation. In the worst cases, untreated mental illness leads to death – of parents and sometimes, their children.
The WHO Mental Health Action Plan 2013-2020, (extended to 2030) endorsed by all national Ministries of Health, lays out four objectives:
Download WHO Mental Health Action Plan
To date, the African continent is behind others in meeting these objectives. For example, only 21% of African countries have recent mental health legislation compared to a global average of 40%, and only 27% have resourced policies, compared to 53% in the rest of the world. The mental health workforce is a tenth of the global average (0.9 professionals per 100,000 population vs. 9 per 100,000 population).
“There is no health or sustainable development without mental health; mental health is too important to be left to the professionals alone, and mental health is everyone’s business.”
WHO Mental Health Action Plan

Initiating a Local Response in the Ukwega Ward
In my position as Global Volunteers Co-Founder, I led the first service program back to Tanzania since the beginning of the 2020 global pandemic. Two years earlier, I asked our program host, Bishop Owdenberg Mdegella, whether assessing the community’s interest in mental wellness support within the RCP Program would be an acceptable project. Because mental health in Tanzania is a stigmatized topic – as it is around the world, I was concerned about raising a potential taboo. The Bishop asserted that behavioral health is critically important to local people, and the community would be open to conversations. With that assurance, in November 2018, I met with village leaders, secondary school teachers, and RCP caregivers in addition to three families with children living with mental illness to understand their desire for mental health education and care. Unilaterally, the RCP families of the Ukwega Ward encouraged Global Volunteers to work with them on a community mental wellness program.
Over the two years since those first meetings with community leaders, I investigated a number of approaches to presenting mental wellness education to RCP families. Through my research into WHO, U.N. and Tanzanian mental health resources, I developed seven initial workshops for review by our Tanzanian medical collaborators. These were consolidated into four after consultation with staff on the ground, and further refined to address local questions and interests. Each workshop presented topics requested by RCP parents and community leaders; many of which I had personal knowledge. Broadly, the workshops covered the cause and treatments of mental illnesses; perinatal and post-partum depression; alcohol abuse and mental illness; and family and community support for mental wellness.
The scope of perinatal depression in the RCP villages hasn’t been documented, but it is believed to be prevalent, based upon anecdotal reports at the IGC and during home visits. According to WHO, worldwide about 10% of pregnant women and 13% of women who have just given birth experience a mental disorder, primarily depression. In developing countries, the percentage reaches 16% during pregnancy and 20% after childbirth. In severe cases, their babies may become malnourished or neglected because the depressed mothers cannot function properly. Prolonged or severe mental illness hampers the mother-infant attachment, breastfeeding and infant care. This is one of the paths to childhood stunting, and on occasion, untreated depressive psychosis leads to maternal suicide and/or infanticide. Effective interventions, delivered by well-trained, non-specialist health providers can circumvent such tragic outcomes.

Because treating maternal depression improves the growth and development of the fetus and the newborn, the RCP Program seeks to reduce the incidence of prenatal and post-partum mental illness. The corresponding workshop and caregiver follow-ups with self-assessments at home visits cover the causes, symptoms and treatments of post-partum depression, and the role of the family and community in supporting the mother and child. We’re grateful to engage the guidance and support of compassionate clinicians at regional medical facilities as we scale up our initial efforts.
“We are ready and able to share our ideas and the resources we have (at Iringa Region Referral Hospital) in helping the society in solving different mental illness problems,” asserts Dr. Yusto Kinyoa, a psychologist, Lutheran pastor and mentor for psychology students from the Universities of Dar es Salaam and Iringa. “We wish to ensure good mental health to everyone at Ipalamwa based on the WHO-CBT manual and to help achieve the biggest project of RCP in collaboration with you.”

Likewise, alcohol abuse is rooted in chronic stress, trauma, poverty, anxiety, depression, low self-esteem, isolation, physical and mental disorders and and a family history of addiction – all characteristic of developing communities. These are the same conditions leading to childhood and generational stunting. Alcohol abuse in the rural areas of Tanzania is a significant concern, and its impact on physical and mental health is well-known. But the connection between alcohol abuse and mental illness isn’t widely recognized by the same population. WHO estimates that about 50% of people with chemical abuse problems have a co-occurring mental illness. The workshops instruct parents how chronic alcohol abuse compounds anxiety, depression and the psycho-social problems that accompanies those conditions. They learn that many of these negative effects occur at low doses of alcohol, and can cause impaired judgment, cognitive problems, and reckless behavior that results in personal injury or spousal and child abuse.
The workshops place the family and the community in the center of harms reduction and recovery. Strengthening social support is the first step in a community-based mental wellness program. RCP parents are encouraged to assess their immediate family support and community connections. Community and religious leaders are challenged to look for ways to deepen meaningful outreach to struggling community members and to open discussions on mental health in Tanzania.
“We wish to ensure good mental health to everyone at Ipalamwa based on the WHO-CBT manual and to help achieve the biggest project of RCP in collaboration with you.”
Dr. Yusto Kinyoa, psychologist, Iringa Region Referral Hospital
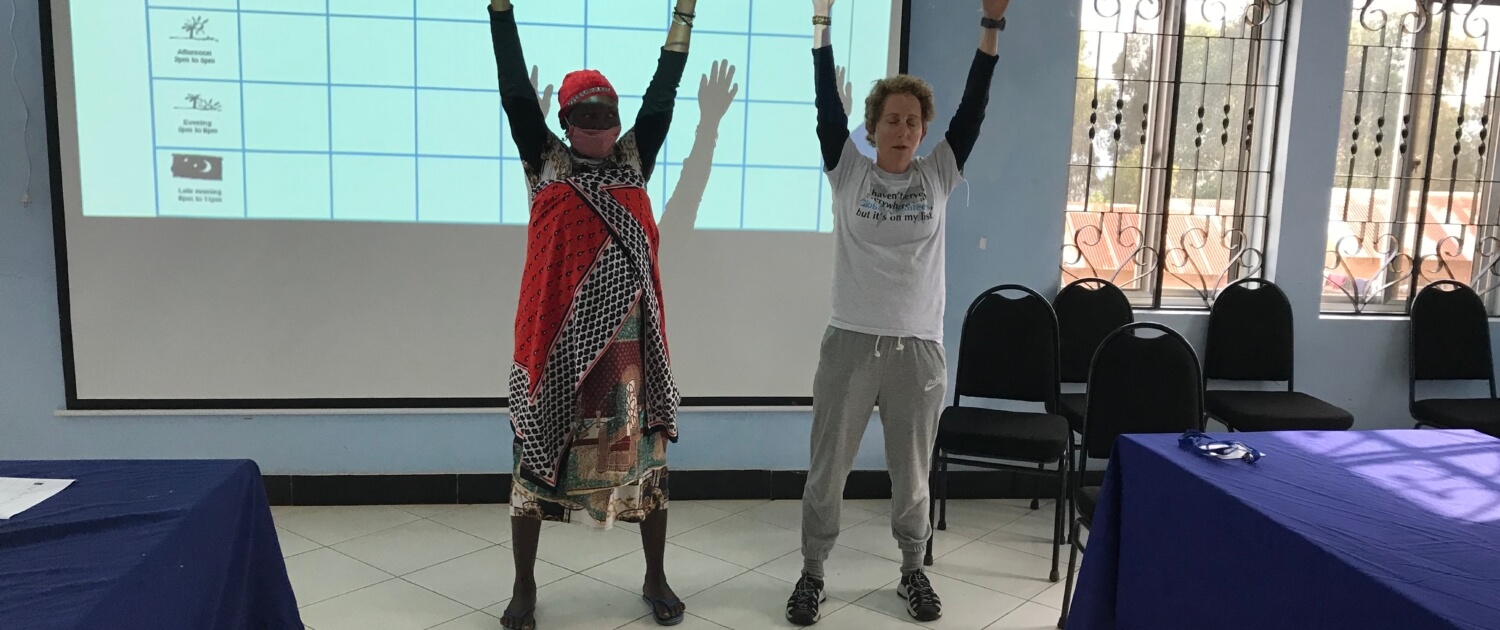
Finally, we demonstrate accessible stress-reduction practices such as yoga, deep breathing and mindful reflection with the introduction of healthy responses to anxiety and depression. Together with behavioral health self-assessment tools, RCP caregivers are reinforcing these new concepts during home visits and encouraging any individuals with questions about their own mental wellness to discuss their concerns with IGC doctors, who can provide diagnoses, prescribe medications, and refer patients to specialists in regional hospitals who collaborate with RCP.
“In order to achieve all this, we need to decentralize mental health services into primary care, where is the base and catchment area.”
Dr. Petro Lusasi, psychiatrist at Ilula Lutheran Hospital
“Goal 3 of SDGs is to ensure healthy lives and promote well-being for all, at all ages. In order to achieve all this, we need to decentralize mental health services into primary care, where is the base and catchment area,” says Dr. Petro Lusasi, psychiatrist at Ilula Lutheran Hospital, which is one of the referral hospitals for RCP families. “Target 3.4 of the SDGs is by 2030 to reduce by one third premature mortality from non-communicable diseases through prevention and treatment and promote mental health and well-being.”
We have great optimism for the development of a robust mental health component in the RCP Program over coming years, and the emergence of an model of integrated physical and behavioral community wellness for the region and the country. Mental health in Tanzania can be accessible with volunteers’ assistance. Join an upcoming service program to contribute!


Leave a Reply
Want to join the discussion?Feel free to contribute!